Fifth in a series looking at serious issues with emergency health services in British Columbia.
If you have a story to share with us about your experiences, send an email to newsroom@castlegarnews.com.
Advocates of an improved pre-hospital care system argue that the overall costs of adding more ambulances, paramedics, helicopters and fixed-wing aircraft to British Columbia’s emergency health-care system would be countered by the savings generated from shorter hospital stays, less time spent in rehabilitation facilities, lower disability claims, etc.
“From a cost perspective alone, all the politicians from all of the parties should be tripping over themselves to put together a vastly more capable pre-hospital care system,” said Hans Dysarz, executive director for the advocacy group . “It is literally bleeding our health system out.”
What is often referred to as the golden hour — the first hour following a traumatic injury or illness in which prompt treatment is most likely to make a difference in preventing death or dire outcomes — is often used up in rural B.C. before a patient ever reaches a hospital.
Missing that golden opportunity for treatment can result in extended hospital stays, need for long-term care and permanent injuries leading to disability claims — all which cost the medical system.
According to the Provincial Health Services Authority, the yearly cost of injury exceeds $2.8 billion in B.C.
Over 700,000 people are injured yearly in B. C. Of these, approximately 1,800 die, 9,000 suffer permanent disability, 27,000 are hospitalized and an estimated 41,000 potential years of life are lost. (Trauma Services BC)
The Public Health Agency of Canada reports that in 2010 the total economic burden of injury across the country was $26.8 billion, of those costs, $15.9 billion was health-care expenditures and $10.9 billion was associated with reduced productivity from hospitalization, disability and premature death.
The costs of injuries have been climbing each year, so current numbers are likely a lot higher. These figures are only for injuries and do not include other urgent medical issues such as strokes or heart attacks — two situations where timely treatment is of utmost importance.
So the question many are asking is: “Wouldn’t an investment in better pre-hospital care reduce those figures — lowering costs, permanent disabilities and lives lost?”
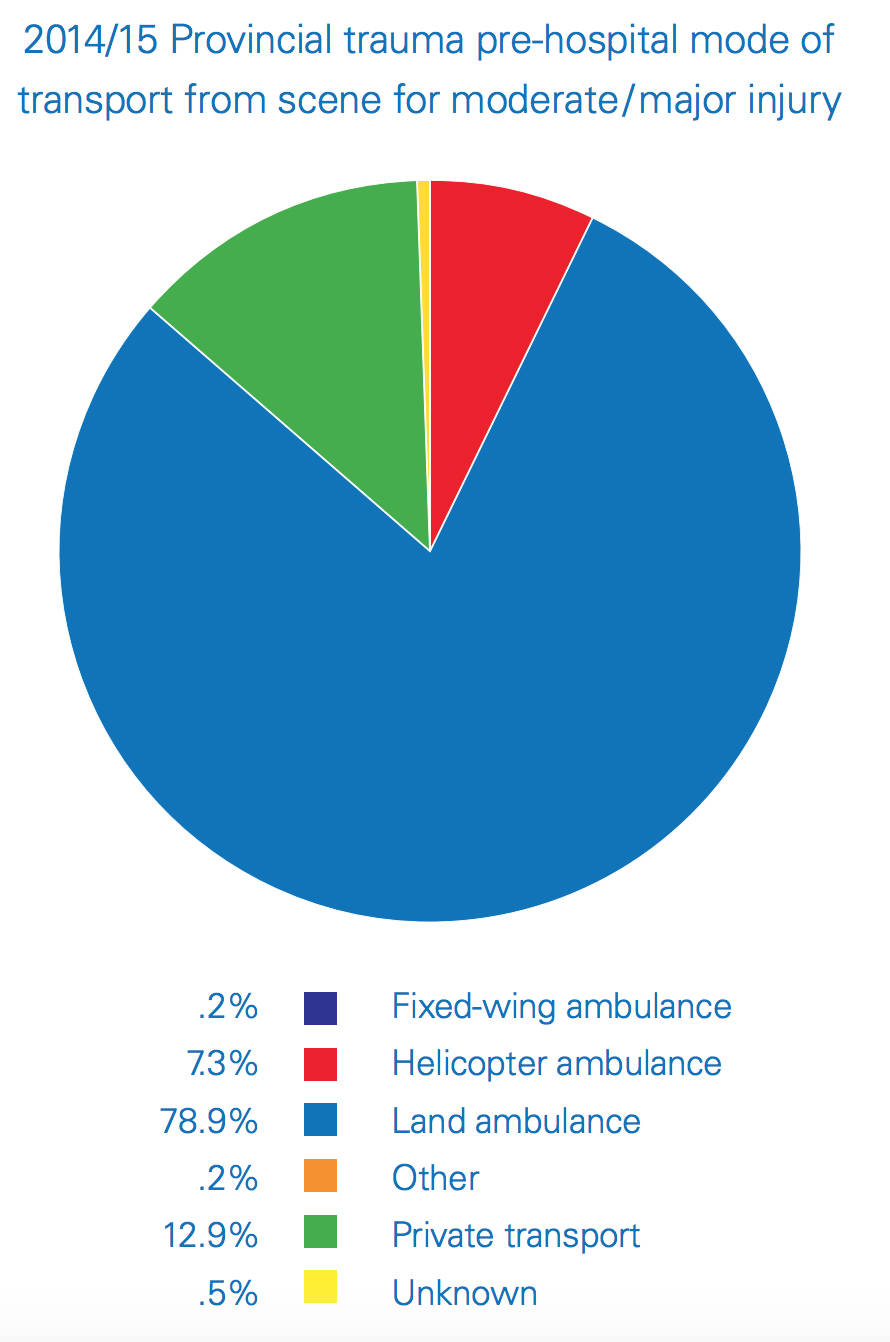
When transportation is primarily done by ground ambulance, more than one million rural B.C. residents are so far from a trauma centre that transportation time alone takes so many hours that sometimes opportunities for improved outcomes are lost.
This is combined with the fact that almost all of the ambulances transporting those patients are Basic Life Support ambulances which are limited in equipment and not staffed with paramedics at the highest level of certification.
All three of B.C.’s Level 1 trauma centres are located in the Vancouver area. The Level 2 trauma centres are located in Kelowna, Kamloops and Victoria. Three of the Level 3 trauma centres are located in the Lower Mainland, one in Nanaimo and one in Prince George. That leaves a vast swath of B.C. residents with a very long way to travel to reach the help they need.
“Yet all of B.C.’s rural residents help to pay for these facilities and highly skilled staff year after year,” stated Dysaryz. “That is a form of taxation without representation — or in this case, taxation without timely access. And rural residents are dying and ending up with permanent injuries as a result,” said Dysarsz.
The long distances to hospitals designated as trauma centres are one of the reasons why BC Forest Safety Ombudsman Roger Harris called for the province to add more air ambulances to its emergency health care system in a recent .
In Harris’s report he says, “When all factors are considered, HEMS (Helicopter Emergency Medical Service) may, in fact, be more cost-effective than ambulances in the total overall cost to the health-care system when you factor in patient outcomes to the equation; and second, if you apply the logic of using low call volumes as a determinant of allocating emergency medical resources to an area, then conceivably a community with little or no crime or fire could find themselves without those services as well. It simply is not a reasonable argument to make.”
The report continues, “There are no technical, or infrastructure barriers to the delivery of helicopter emergency medical services within that critical first hour to each and every resident of B.C., regardless of where they live. The decision by the government not to provide those services is a choice.”
“Faster care results in less overall health care costs,” states Harris. “It is an accepted fact the quicker an accident victim can access medical care, the better the medical outcomes, the shorter the period of time for rehabilitation resulting in an overall lower cost to the health-care system. As emergency response is one component of the cost, investing more in ensuring patients receive timelier treatment, could result in overall savings to the cost of moving a patient through the system.”
Alberta’s air ambulance service STARS estimates that: “Timely treatment of stroke, heart attacks or brain injuries can save more than $1 million per patient. The economic benefits of helicopter ambulance missions are six times higher than the costs.”
Every time an outcome is improved, the costs go down. A regular hospital stay costs less than an ICU stay, a temporary or partial disability costs less than a full disability and every day shaved off of a hospital stay saves thousands of dollars.
An out-of-province perspective
The Castlegar News heard from an Ontario paramedic leader with over 30 years of experience who is very concerned about the state of pre-hospital care in British Columbia.
He shared that he has many friends in the British Columbia Emergency Health Service that are afraid to speak out about their concerns due to potential repercussions, so he has made a commitment to his B.C. paramedic friends to advocate for better service for B.C. residents.
This paramedic has worked at the primary care and advanced care levels, in ground ambulances and on helicopters and in both urban and rural areas.
He is advocating for more ambulances and paramedics, more helicopters and planes and more equipment on board, especially ECG monitors.
In B.C. primarily only Advanced Life Support (ALS) ambulances staffed with Advanced Care Paramedics (ACP) have ECG monitors on board. The total of ALS ambulances in the province is less than 30. Other provinces utilize ECGs much more extensively in ambulances staffed at the Primary Care Paramedic (PCP) level.
“Equipping PCP crews with the tools that every other province does makes financial and moral sense,” explained the Ontario paramedic. “The rest of the country considers [ECG] a staple tool required to do the profession.”
“Cover the province with a net of well-trained paramedics in both fixed wing and helicopters and survivors will be lining up to say thanks,” he added.
He also stressed that paramedics should not be looked at as just a means of conveyance — they should be treated as a huge part of the medical team.
In his experience in Ontario, PCP paramedics daily diagnose patients having critical cardiac arrhythmias, treat the patient with oxygen and ASA and then based on a 12 Lead ECG either redirect the patient to a cardiac center for emergency surgical intervention — bypassing emergency rooms — or in the absence of a cardiac centre, alert the hospital of an inbound patient with clinically significant 12 lead changes so that the “door to drug” time can be reduced.
“This in no way is meant to disparage the hardworking staff at BCEHS,” he said. “But it is time that the government look at what the rest of Canada is doing and start being a leader instead of bringing up the rear.”
Personal stories
Castlegar News has been approached by people who wanted to share their personal stories related to ambulance services — here are two of these accounts.
One woman shared her family’s experience after her mother became ill in 2016. The patient ended up in the hospital and needed surgery for a blockage in her stomach. The surgery was performed, but the next morning the patient was in critical condition and moved to ICU.
“She was not there long before they contacted Vancouver and called BC Ambulance Service for a transfer,” added the patient’s daughter.
She reports that the call for an urgent transport was made before noon and the critical care team arrived shortly after 2 p.m. It was after 4 p.m. when the patient was flown out of Trail and arrived at Vancouver General Hospital just after 6 p.m.
“My mother was rushed into surgery shortly after she arrived but sadly passed away two days later,” said the patient’s daughter. “My mother’s hepatic artery proper had been damaged in the first surgery and her organs were starved of blood flow.”
“Maybe if it didn’t take six hours to transport her to Vancouver she might have been saved.”
She questions the purpose of having a helicopter pad at Kootenay Boundary Regional Hospital if it is seldom used — last year there were five helicopter transports in Trail.
“Why did we donate and raise $800,000 for a helicopter pad if we don’t use it?” is one of many questions she has about why it took six hours to transport a critical high-priority patient.
The nearest helicopter operated by BCEHS is stationed in Kamloops.
BCEHS has stated that helicopters are sometimes limited in flying capabilities based on the weather — it is unclear whether that was a factor in this situation.
Asthma attack
Another woman shared her story about what happened when she called for an ambulance when her husband was experiencing a “critical life-threatening asthma attack.”
“The crew did an amazing job in relation to their limited training and limited scope of practice,” she said. “But my husband had minimum air entry and needed a medicated nebulizer immediately that they weren’t able to administer.”
She reports that the crew was proactive and contacted another BCEHS crew with higher levels of training, but the ambulance had to drive 30 minutes before meeting up with the second ambulance and before he was given medicated treatment.
This was then followed by another 30 minutes of driving to get to an emergency room because the emergency room at the hospital nearest where they live is not open during evenings and weekends.
“When you can’t get air into your lungs that is a long time to wait,” added the patient’s wife.
“If Interior Health is not going to provide emergency care 24/7 to B.C. residents, then first-time responders should be at the highest level of scope of practice in order to provide life-saving treatments and medication to patients in a timely fashion,” she said. “This training/education should be made available to the present dedicated BCAS personnel.”
“B.C. emergency care and first responders need to be modernized from their present 1980 model so that lives are saved and prolonged suffering for patients isn’t endured any longer,” she added when sharing her frustration.